Day 3 - Hypercalcemia
Pillars of Management
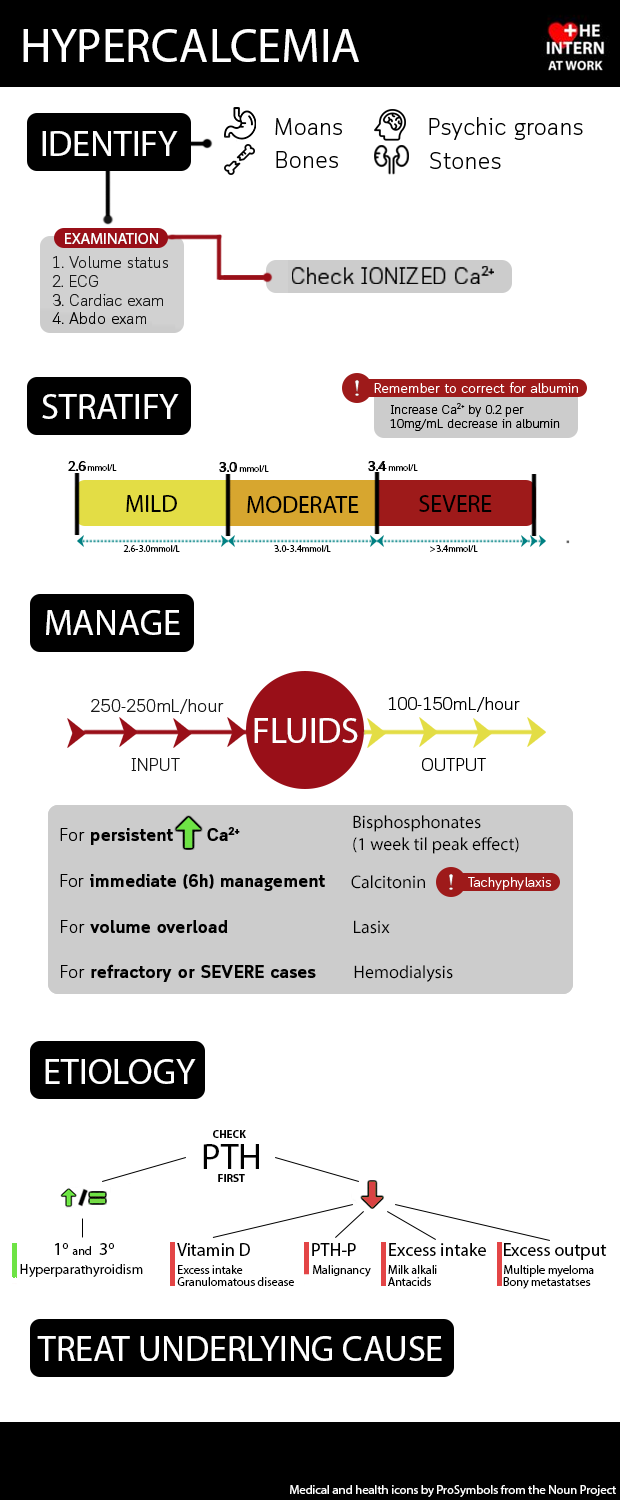
Calcium < 3.0mmol rarely causes symptoms
Volume resuscitation
Goal is to maximize urine output with aggressive IV rehydration
Administer 1-2L normal saline bolus then continue 200-250mL/hr to target urine output 100-150mL/hr
If there are concerns about volume overload can administer furosemide IV to facilitate ongoing volume administration
Treatment of underlying cause
Discontinue medications that cause hypercalcemia ie. supplements, lithium, thiazide diuretics, vitamin D
Investigate potential causes and treat where possible, ie. multiple myeloma, hyperparathyroidism, bony metastases, tuberculosis, sarcoidosis
If ongoing severe hypercalcemia:
Calcitonin - 4units/kg/day in 2 divided doses for immediate effect (works within 6hrs)
Will develop tachyphylaxis within 36-48hrs, therefore, used to temporize but not for ongoing management
Bisphosphonates - pamidronate 60-90mg IV or zoledronate 4mg IV
Requires 24-48hrs to take effect, reaches peak effect within 1 week
Consider corticosteroids ie. prednisone 10-40mg po in granulomatous diseases
If refractory severe hypercalcemia or unable to tolerate fluids, consider hemodialysis