Day 1- Approach to Acute Monoarthritis
Approach to Acute Monoarthritis (CMAJ)
Must rule out septic arthritis !
If there is a concern for septic joint, administer empiric antibiotics (ceftriaxone 2g IV + vancomycin 1g IV) and preform arthrocentesis
Gout/CPPD:
Acute management:
NSAIDs: naproxen 500mg PO BID until acute episode resolves + colchicine 1.2mg PO once then 0.6mg PO BID (d/c 2-3 days after episode resolves)
Use corticosteroids (prednisone 30-50mg taper over 7-10 days) if NSAIDs/colchicine contraindicated
Contact rheumatology for potential intraarticular steroid injection
Emerging evidence that irate lowering therapy may have a role during acute gout flare (if patient meets indications)
Long term managment:
Urate lowering therapy (if indicated)
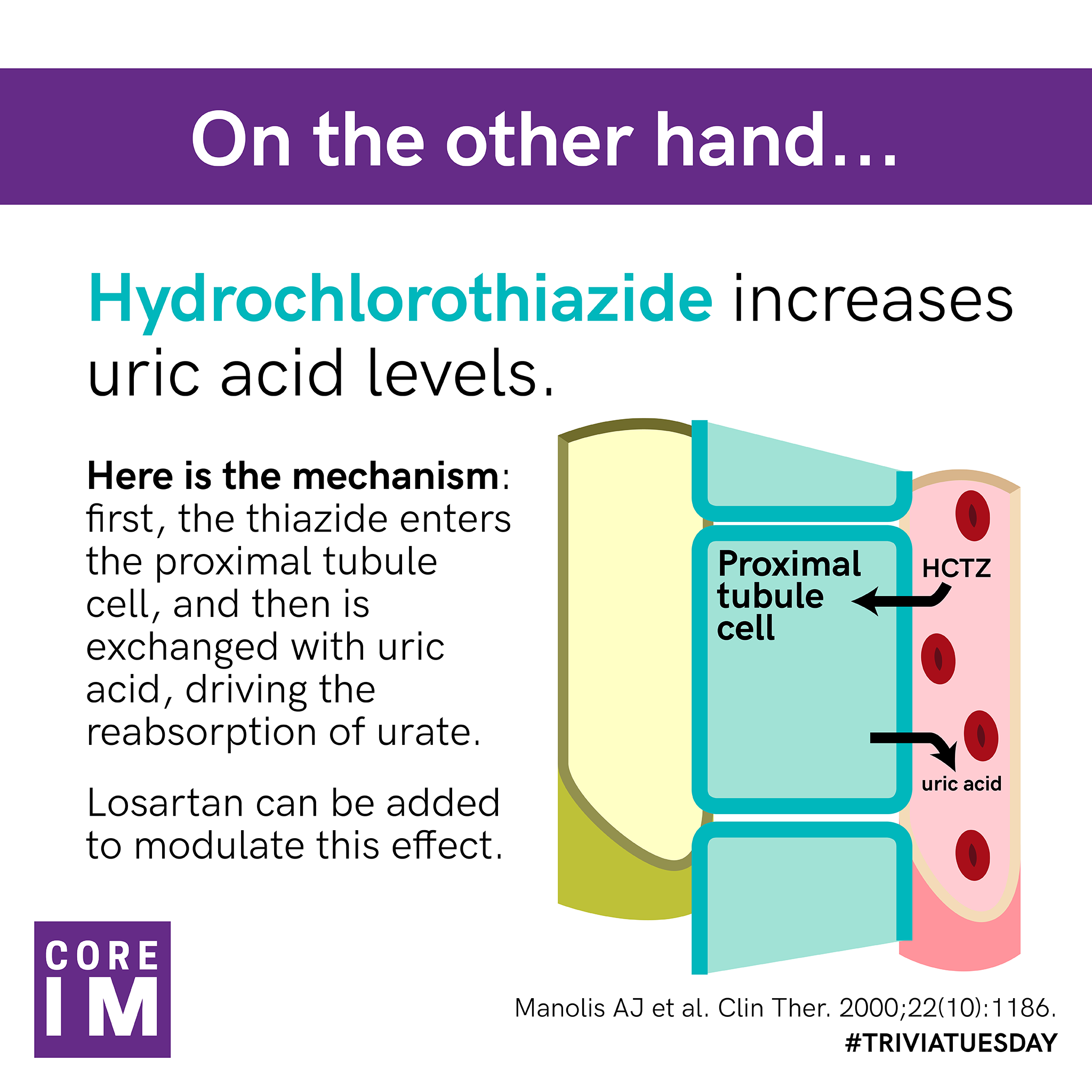
For comorbid HTN, avoid hydrochlorothiazide, use losartan (has an independent effect to lower uric acid)
Gout friendly diet (see graphic)